Social cooking
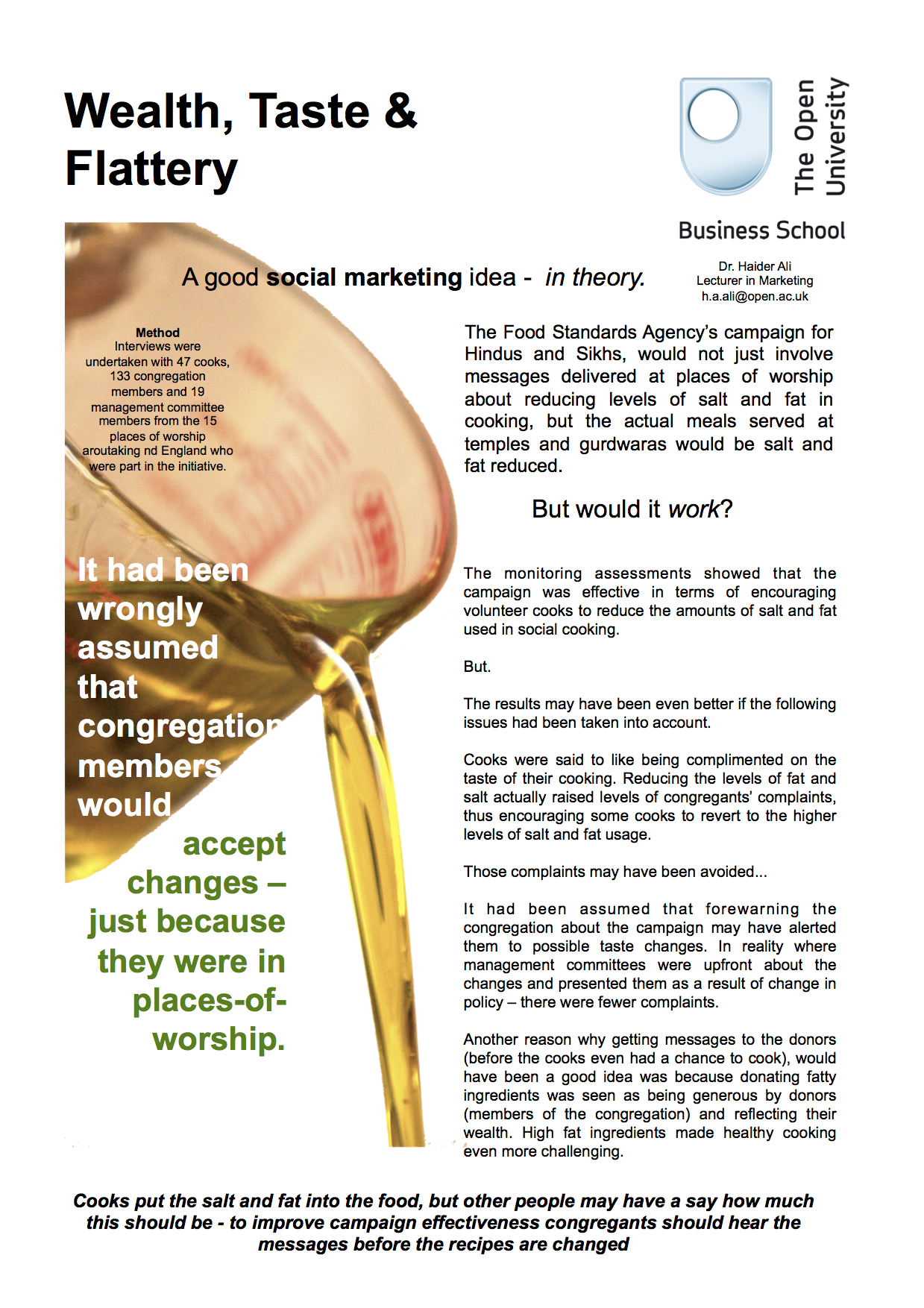
The British Heart Foundation and the Food Standards Agency sought to encourage the preparation of healthier meals and this was undertaken as part of their 'Social Cooking' project. Further details on the left of this page.
HeartNet
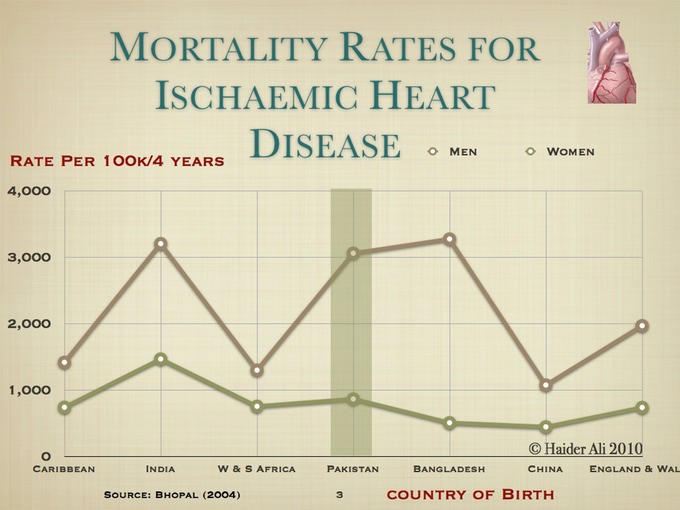
Higher incidence of Coronary Heart Disease amongst some ethnic groups
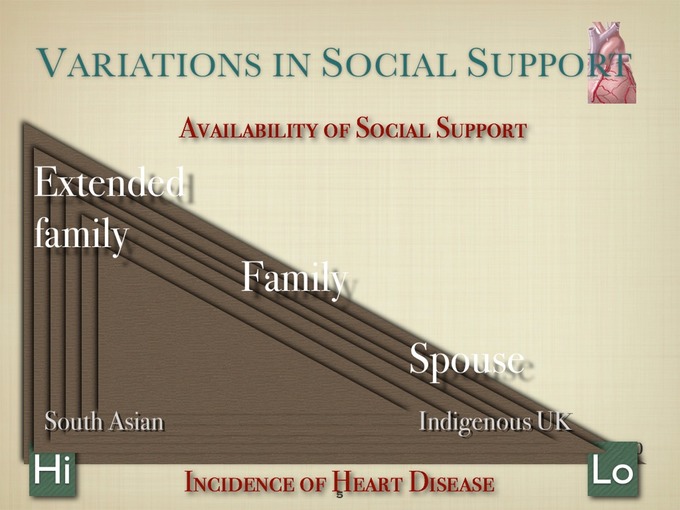
People of South Asian origin (people with ancestry from India, Pakistan, Bangladesh and Sri Lanka), have a higher propensity to CHD than the UK population in general (Wild & McKeigue 1997). Furthermore there are also evidences suggesting a higher prevalence of cardiac risk factors (such as insulin resistance, diabetes and high cholesterol) and cardiac risk prone behaviours (such as, obesity, low physical activity, smoking and high fat diet) among this population. The lower levels of knowledge and understanding of CHD risk factors in these communities compound this problem (Datta 1995).
There is also a lower level of uptake of services within these communities (Mc Keigh & Miller 1998) and compliance with drugs regimes. In particular research shows that the first generation of immigrants have higher levels of mortality attributed to heart disease than other population groups (Balarajan 1996).
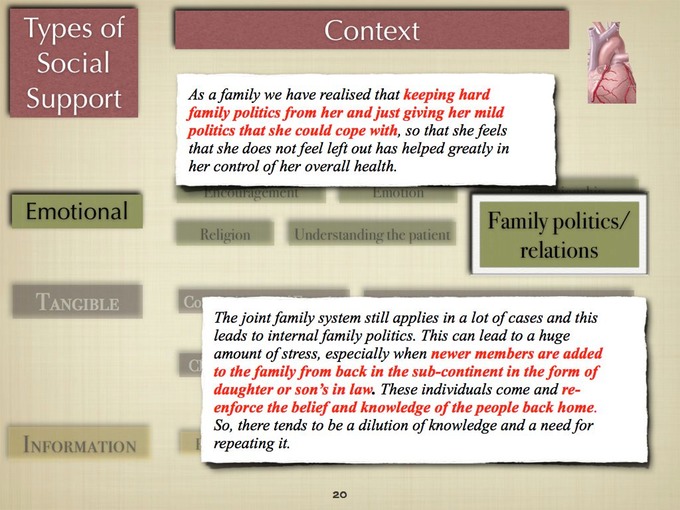
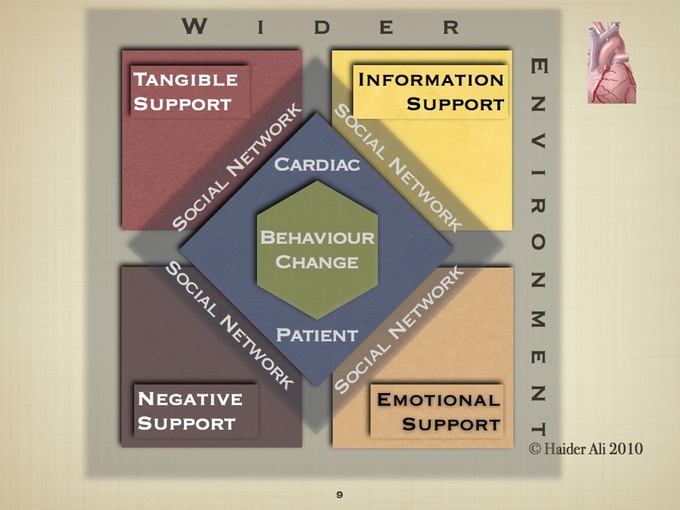
Culture & social support and cardiac patients' lifestyle management
Given the problems faced by this minority ethnic group, the purpose of this research has been to gather insights into the way in which social support is provided by friends and relatives to cardiac patients of South Asian origin. In particular we have focused on South Asians of Urdu speaking origin, who are originally from Pakistan. For this research we have also gathered data from other ethnic groups in order to throw into sharper relief how Asian cultural norms may have changed or adapted to the British context.
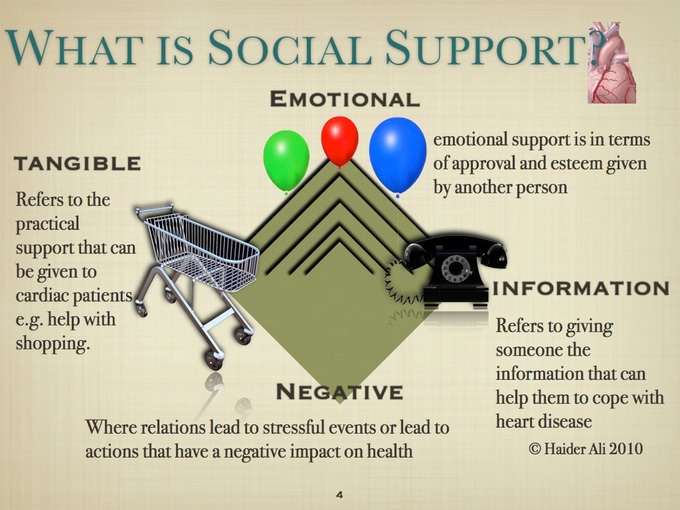
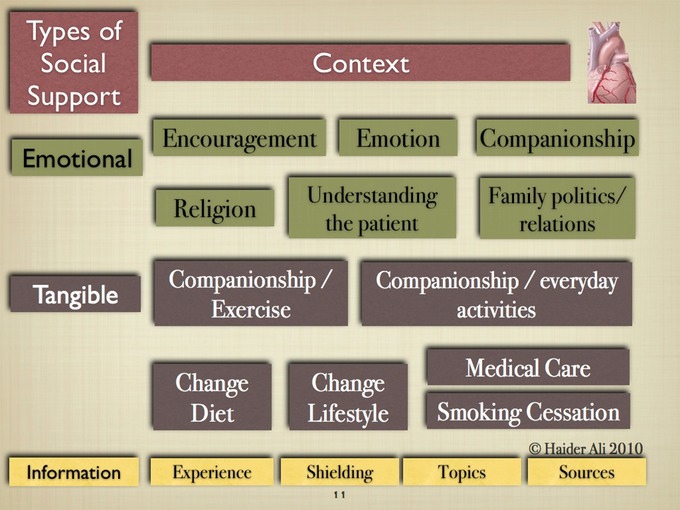
Cardiovascular disease and social support
Social support is supposed to be protective of cardiovascular health. This is supported in cross-sectional and longitudinal population studies, in intervention studies with humans and animal experiments (Kristina Orth-Gomer 1994).
In multivariate analyses controlling for standard risk factors (blood pressure, lipids, coagulation factors, family history, sedentary lifestyle, etc.) two factors emerged as the strongest independent risk factors for MI in middle aged men: smoking and lack of social support (Orth-Gomer, Rosengren and Wilhelmsen 1993). This was the first study to prospectively link social support to the occurrence of heart disease.
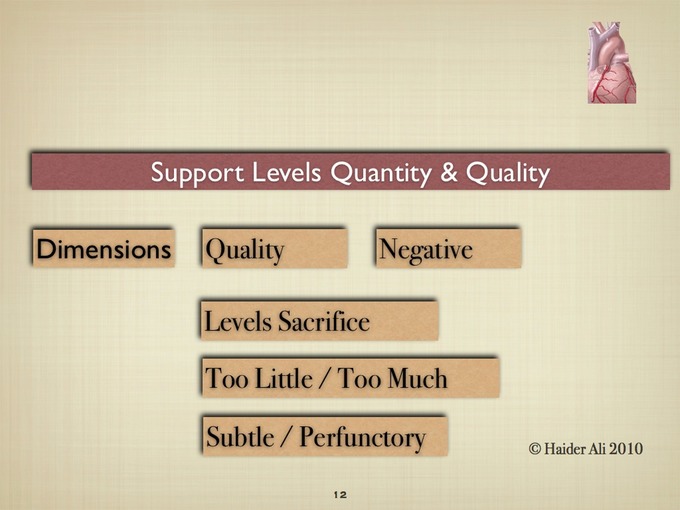
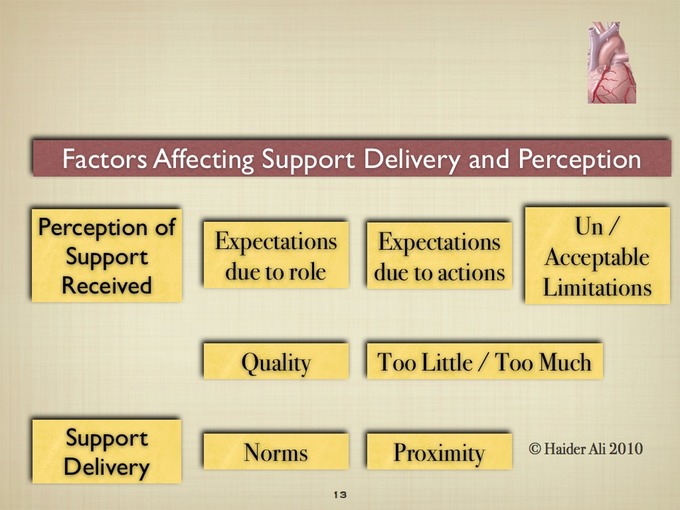
Frequency of social contacts, the number of available persons and the amount of social activities seem to have a substantial effect on health and survival. If size and density of social networks have an effect on health this could be due to qualitative rather than quantitative characteristics of the social interaction. Also social interaction if improper could be a stressful factor in itself and may promote rather than inhibit illness. Recent studies have sought to develop qualitative measures that could tap into those aspects (Orth-Gomer & Unden A-L 1987). Stansfeld (1999) argues that a richness of analysis may be obtained by examining the quality of support as well as the social network.
The following presentation was made to the European Marketing Academy Conference (2007) in Reykjavik.
Healthy Ramadan Campaign
The messages to be delivered by the campaign focused on the importance of managing salt consumption within an overall healthy lifestyle that includes stopping smoking and reducing fat consumption. By delivering a prominent message about salt consumption within the framework of a wider campaign the aim of the campaign was to deliver the salt message to a wider range of people, using a wider variety of media than would otherwise be possible.
The target for this campaign were Muslim communities, these are people originally from the following countries, Bangladesh, Pakistan, India, Afghanistan, Turkey, Iran, Algeria and a significant number of African and Afro-Caribbean people. It has been estimated that there are about 1.5m Muslims living in Britain, about two thirds of whom are of South Asian origin (Weller 1993). Pakistani, Bangladeshi, Turkish, Kurdish and Somali communities form the majority of the Muslims communities in the UK and they are also most deprived.
One of the drivers behind the campaign was the relatively high levels of smoking in various Muslim communities in the UK. A presentation linked to this work is here.
Faith leaders and workers
This was a training programme (sponsored by CLG - (a UK government department) aimed at faith leaders and workers and the social marketing element was the emphasis on encouraging interfaith dialogue and better governance in places of worship as a means of combating extremism. My colleagues and i assessed the programme and the report can be accessed here.
Publications in social marketing